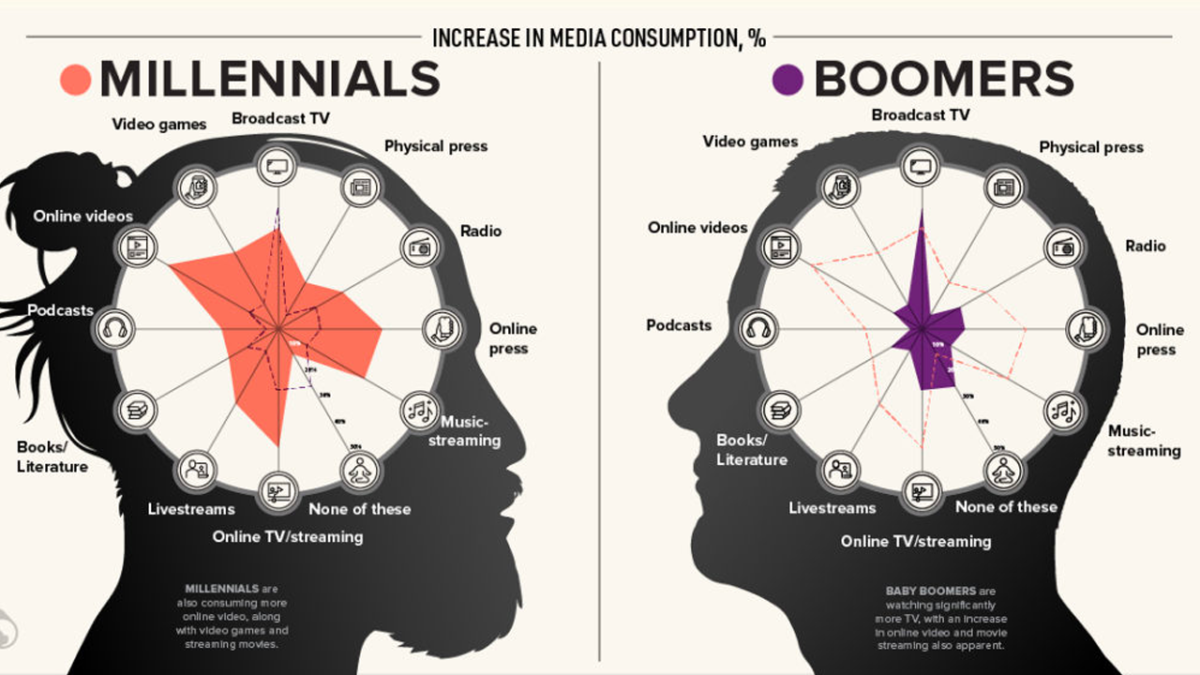
As a physician and public health doctor, sometimes I wish that some of the articles that are available to digest by the avid online reader about COVID-19 carry a disclaimer: Read this at Your Own Risk.
We have been bombarded by information on various media outlets during the COVID-19 pandemic: some of it is accurate, some of it is conjecture; some of it is instructional, and some of it is proverbial snake oil. As we comb through this information, we build a narrative of an otherwise great unknown that is unraveling in real time. Statements given with some assurance are walked back after more information is gathered from epidemiologic studies and research – which too are subject to challenges of interpretation. First no maskes, then masks; the epidemic is controlled versus it is an uncontrolled pandemic. It causes mostly mild disease versus it is a “fatal” virus. The shift in words begin to shape a different realities, one of which is of hopeful optimism and acceptance, another of growing distrust and even fatalism.
Our brains are intrigued by natural phenomena Photo by Nastasya Day on Pexels.com
Our realities are as much factual as they are individual or group narrative. Reality is shaped by our senses and higher levels of cognition, which apply meaning or weight to information, accepting or discarding it to shape a narrative. Just like we can be fooled by a two-dimensional object spinning on the paper, so too can our higher levels convince us of a possible reality that is inaccurate. We don’t always know our blindspots in this either. These blindspots that affect our reality are known as biases.
Even as we click on articles, there is a natural, confirmation bias, applied to the titles of studies or reports that we would read. To some extent, a story was already starting to take shape in our minds before further information is available to disprove it – and even afterwards, we discount that new information. This is known as anchoring bias. It is in the current time of media frenzy that a structured approach is useful to gain a greater sensitivity in the biases that shape the messages we read and the stories journalists tell, to enhance our approach to detecting the reason of the article (instruction, narrative shaping, fear mongering), and to determine the validity of the article.
**Read This at Your Own Risk**
Myths that are currently circulating in the news:
The virus was engineered to be more lethal in causing a pandemic and was leaked out of a high security lab in Wuhan, China.
The Chinese government deliberately released the virus onto its population and the rest of the world to create instability, so that at a later point, they could reap the benefits economically.
Information about the COVID-19 is deliberately being withheld to the public to have control over the population. This could have several extensions: the government is forcing doctors to code deaths as related to COVID-19, so that it can inflate the death statistics or doctors are incentivized to code deaths as related to COVID-19, because they receive a higher reimbursement (not exactly the reason).
The possible stories are as endless as the imaginations that construct them. Once these ideas are framed, our brains will start building this alternate reality by looking for material that supports it, while negating material that opposes it. Commonly, these stories rely on assumptions that large groups or governmental entities would need to keep a secret from others or be consistent in their actions. The other common fallacy is the requirement that multiple unproven, unplausible suppositions would need to be true in order for the endpoint to be true. This is known as the Narrative fallacy. When one point is disproven or pseudoscience, then all of the dominoes fall.
TheDunning-Kruger Effect: bias that leads people of limited skills or knowledge in a topic to believe mistakenly that their abilities are greater than they are. One example that I see in the clinic is “Dr. Google,” where someone, after doing a google search on their symptoms and reading a few articles, has been able to diagnose themselves with a rare disease and speaks as a specialist in the field.
Brainwashing: This refers to the “read at your own risk” disclaimers. The idea is that somehow information online could completely persuade someone or radicalize them after reading it. Fortunately, we can prevent this from happening and put on our cognitive goggles to dampen the power of suggestion (see below article link).
Deliberate Ignorance: This is a fallacy where one’s mind is made up and they refuse to listen to additional information that may change their conclusions. “Don’t try to confuse me with facts, my mind is made up!”
The Big Lie Technique: This is directed toward a deliberate practice. It is a concept of repeating half-truths over and in different forms until it becomes accepted as truth. Some of the narratives that have emerged during the pandemic have developed from repetition of half-truths or initial information as well, such as the efficacy hydroxychloroquine, but this was not deliberate – pointing to more to an Anchoring bias.
Suggestions on how to interpret the Media
“Let me control the media and I will turn any nation into a herd of pigs.” -Nazi Propaganda Minister, Joseph Goebbels.
“If you tell a lie big enough and keep repeating it, people will eventually come to believe it.” Joseph Goebbels. (Example of The Big Lie Technique)
“He who controls the media controls the minds of the public.” Noam Chomsky.
“How do we know that two and two make four? Or that the force of gravity works? Or that the past is unchangeable? If both the past and the external world exist only in the mind, and if the mind itself is controllable – what then?” George Orwell
Joseph Goebbels, the Nazi Propaganda Minister fed lies and half-truths to the public by fashioning media messages, in order to garner support and appease concerns during the Third Reich. Although not as deliberate of an action nowadays, any news that we read can have a subtle or explicit narrative that shapes our perspectives. The media has the daunting responsibility to ensure that the information provided to the public is informative, free of bias, and does not breed misinterpretation.
The cognitive biases that fuel our narrative, allow us to detect patterns, and even think creatively “outside the box.” Although we cannot (and need not) completely escape our biases, a greater sensitivity to them and understanding of the red flags for narrative traps can protect us from untruths and hone our resilience from the harmful states that result from negative, sensationalistic news: where fear develops and triggers the self-preservation instinct of fight, flight or freeze, resulting in a negative impact on our bodies.
I had the opportunity to collaborate with a friend and colleague, author and founder of Becoming Better People, Jacqueline Jannotta Rothenberg. She is an excellent writer and author of Let’s Leave the Country!. She wrote an article about our interview along with her insights, which provides instruction on how to address the media storm amid the COVID-19 pandemic and how to keep what Jacqueline refers to a “good media diet.” The link to her website is embedded in the title that follows.
I leave you with this message from C.S. Lewis, one that was communicated through the poignant art of seventh grader Yara Kanar (The Second Cov-Art Children’s contest) In the middle of a global outbreak, its empowering to think that each of us can shape the way this story ends through our actions and our interpretations.
Currently over 4,700 covid-19 deaths in New Jersey have occured in long-term-care facilities so
I am very motivated to do what it takes to stay in my home. For example, my cleaning lady has not come for 6 weeks because of the pandemic. When I smelled dust and started to sneeze I felt compelled to try vacuuming until it is safe for Isabel to be in my home for two hours.
I vacuumed years ago so I already knew 2 tricks. (1) Vacuuming is exhausting because it requires stepping forwards and backwards abruptly a hundred times so I vacuum only one room a day.
(2) I knew tripping on the cord was a huge fall hazard. Thankfully I can hold the cord out of my way. I rest the cord in my partially curled hemiplegic fingers and use shoulder abduction to hold the cord away from my body.
I discovered 2 new tricks to make vacuuming easier. (3) I do not step forwards and backwards.
I stand still and move the vacuum forward and backwards only one arm’s length. Then I take two steps sideways to clean a two-vacuum wide path before moving forward. Most of my falls have happened when I step backwards but I feel stable when I step sideways. (4) Instead of vacuuming in parallel rows the way people cut grass, I start by vacuuming around the perimeter of the room and gradually work towards the center. Making 90 degree turns is easier than 180 degree turns. homeafterstroke.blogspot.com
Nature provides a palette of foods for all palates.
If your only adventure into eating green beans is opening a can of green beans with vinegar and (more) salt, prepare yourself for a paradigm shift: a plate of green been pesto “pasta.”
Green beans are a great food for snacking and in meal preparation. They are replete with fiber and vitamins, particularly vitamin A. Other vitamins and minerals include vitamin C, K, E, niacin, folic acid, iron, magnesium, potassium and thiamine. They have a sweetness that even the pickiest child might notice and enjoy – and come back asking for more.
Is there a difference between the sugar found in vegetables compared with table sugar?
The body reacts to sugar the same way, whether it comes from fruit and vegetables or table sugar. However, that is not the whole story: vegetables and fruits contains intracellular sugar, which means that it comes with a lot of protective fiber. When sugar is processed, it is removed from all of the fiber and is crystallized. By virtue of these steps, this is always going to be greater than what can be encountered in nature.
The sugars (fructose/glucose) in vegetables and fruits are not only found in lower concentrations than processed, crystalline table sugar (sucrose) or processed foods like bread, pasta or pizza, but the fiber and water content, that is taken along with it, affects the amount and pace of glucose absorption in the intestines.
Amount of sugar in one cup note: 4g sugar in 1 teaspoon/1 sugar packet
Natural foods:
1 cup of green beans = 3.3g sugar
1 cup of raw spinach = 1g sugar
1 cup of strawberries = 7g sugar
Processed foods:
1 slice of bread = 14g sugar (in form of complex carbs)
1/4 cup of pasta =14g sugar (in form of complex carbs)
**Take note of the difference in portion between natural and processed foods and remember the fiber and vitamins in the above natural foods.
Preparing Vegetables as a Dish
Green beans can be eaten both raw and prepared. By making it as a plate, you can combine other vegetables and additives, creating a higher level of culinary enjoyment.
Examine the ingredients of Sol Food Nutrition’s Green Bean Pesto “Pasta.” Hazelnuts, tomatoes and basil are added. Some fats are added, including olive oil and cheese. These ingredients add different tastes and textures, along with benefits.
Now on to the recipe! Special thanks to Iris Briand, RDN for providing this savory recipe. She is a colleague of mine who is a dynamic speaker and a great resource to have for nutritional consultative needs. Check out the solfoodnutrition website.
Sol Food Nutrition’s Low Carb Green Bean Pesto “Pasta” Recipe
Ingredients
One large handful of fresh green beans
6-8 dry-toasted local hazelnuts, chopped coarsely
6-10 cherry tomatoes, chopped in half (optional)
Raw parmesan or gruyere, to taste
A few tsp extra virgin olive oil
A few spoonfuls of pesto (optional) – see recipe below, OR fresh basil. chopped
Sprinkle of black pepper and Real Salt (unrefined sea salt)
Preparation
1. Snap off ends + stringy parts of the beans. Then snap them in half.
2. Place a saucepan with steaming basket on stove with high heat and once water is boiling, drop beans in the basket and top it with lid. Turn stove to simmer and let cook for 3 minutes, or until beans are bright green.
3. Shred cheese on cheese grater.
4. Transfer beans to a large bowl and mix in the remaining ingredients. 5. If skipping the pesto step, just add more olive oil, salt, and basil! Enjoy!
Preparation 1. Blend herbs and garlic in a food processor or finely chop. 2. Add oil, salt, and pepper. 3. Toss a few spoonfuls with the green bean mixture! Serve the rest of the pesto with steamed veggies, meat, fish, or homemade veggie burgers! Lasts one week in fridge.
To schedule a FREE 15-Minute Nutrition Phone Consult, please contact Iris
Summary: The COVID-19 Pandemic is an unprecedented event that requires a rift in the societal fabric in order to stop its spread. This forced isolation, along with the threats on financial and health security, can create pressures on those already with a history of depression and anxiety and lead to challenges in those that don’t.
Here are seven tips to nurture your mental wellness and create resilience during this uncertain time of social distancing. Not only will these strategies help you to maintain some normalcy through these times, they just might help you excel.
The COVID-19 pandemic has been responsible for widespread upheaval. Literally overnight, we have been asked to change our behaviors, stay at home other than essential trips out, and wait for this pandemic to pass. Trips, social events, religious gatherings, and restaurants have been canceled or closed. We have been asked to work from home and hold teleconferences instead of physical meetings. For many of us, these are the very ways that we define our social and support network.
Constant reporting of new case numbers and new virus-related deaths has been both emotionally distressing and overwhelming throughout the world. When paired with shelter-in-place orders and the inevitable time spent confined at home, this unprecedented global event has placed tremendous stress on some of the population’s most vulnerable. Current events are making it harder for everyone to protect and promote mental health. Absent of key resources and often unable to receive the same support and social engagement that’s typical of their daily lives, those with diagnosed and chronic mental health issues are finding themselves in an increasingly dangerous space. The good news is that even in times like these, there are still multiple ways to create the conditions for resilient mental health.
Who’s At Greatest Risk Of Experiencing Mental Health Issues During The COVID-19 Pandemic?
Right now and for the foreseeable future, everyone is at risk of experiencing deep depression, anxiety, and stress. So much of what’s going on in the world is impossible for people to control. This sense of helplessness invariably fosters feelings of hopelessness, even in many who have formerly enjoyed consistently good mental health, general mood balance, and overall high life qualities.
However, there is also a very large number of people who are especially prone to mental distress at this time. This includes people who by choice or by circumstance were already spending significant amounts of time alone and in virtual isolation such as: elderly adults with age-related mobility issues, those with agoraphobia or fear of leaving the home, and disabled individuals who largely live in confinement. Those at greater risk for mental and emotional distress at this time additionally include people who are presently battling drug or alcohol addiction, those who have dealt with substance abuse or addiction in the past, recent divorcees, widowers, those grieving close friends, and those with a history of trauma and who may also be living with post-traumatic stress disorder.
Stressors to Mental Health During Quarantine:
A recent review article from Lancet by Samantha Brooks et al. entitled The psychological impacts of quarantine and how to reduce it discussed several risk factors that provoked a greater risk of mental health issues. It is with hopes that identifying the triggers to depression and anxiety can help us to construct ways to mitigate these risks.
Longer duration quarantine (>10 days) or duration uncertain: Associated with poorer mental health, e.g. PTSD, avoidance behavior and anger.
Fears of Infection. In one review, those who were concerned tended to be parents with young children or pregnant women.
Frustration and Boredom. A change in usual behavior even routine things like shopping or social networking can create a sense of boredom and isolation.
Inadequate Supplies Concerns. This includes the ability to get regular medical care and prescriptions.
Inadequate Information. In studies, participants raised the greatest concerns when there was unclear messaging from public health authorities or a concern for lack of transparency. Some concern with adhering with quarantine protocols was a predictor of post-traumatic stress disorder in one study.
Financial Factors. Many people have been asked to modify their work routines such as working from home and, in certain cases, have even lost their jobs. Those with a lower financial safety net, such as those with high debt to income burden, are particularly at risk.
The seven simple strategies that follow can benefit anyone who’s feeling the pressure of world and economic events, and who’s struggling to maintain mental health in the face of prolonged and mandated social distancing and social isolation.
Get Outside And Get Moving
Most shelter-in-place orders that are presently being enforced are not intended to prevent people from going outside entirely. Instead, these orders have been designed to limit gatherings and activities that bring large numbers of people together. Moreover, in addition to not restricting solitary outside activities, or outside activities involving two people or fewer, many of these orders have been issued by municipal bodies that are actively encouraging people to get outside and exercise. The general understanding is that too much time spent indoors and leading a highly sedentary lifestyle is not beneficial for anyone at any time.
Pick a time each day to get outside and get moving. This can be as simple as taking a short walk around your neighborhood or going for a ride on your bike during the early morning hours or late afternoon. Although there are fewer recreational areas still open for enjoyment, there is also far less traffic on the streets. You can use this as an opportunity to better appreciate your neighborhood without the hustle and bustle of moving vehicles and busy consumers.
A short walk or bike ride will lift your spirits and give you the opportunity to re-center your thoughts. It can also make you feel more connected to the world around you. Outside exercise can even be as simple as taking your yoga mat out into the yard or onto a patio or balcony. It might be a good time to get outside to a local park and practice the calming art of Shinrin-yoku, or forest bathing. In addition to benefiting from conscious and structured movement, you’ll have the benefit of fresh air, sunlight, and a restored sense of normalcy.
Continue Interacting With Others Via Social Media And Other Online Platforms
Now is a great time to start making use of social networking platforms. If you haven’t leveraged them before, these are great spaces for reconnecting with distant family members, childhood friends that you’ve lost contact with, and loved ones that you normally communicate with in other ways. Video chat platforms such as Skype can give you the benefit of both speaking to and seeing the people who normally fill your life, and who provide you with the social stimulation and engagement that’s absolutely essential for maintaining good mental health.
Brighten Each Day With Exploration, New Learning, And Other Enriching Activities
For many, the COVID-19 pandemic has provided a very bittersweet silver-lining; massive amounts of free time. For those who are no longer working or having to physically commute long distances to their jobs, as well as those who are no longer attending in-person classes at school, this event offers countless opportunities to engage in new forms of learning and exploration. If you’ve ever wanted to make your own sourdough starter, crochet a blanket for a brand new or aging family member, teach yourself a new language, or pick up the cello, piano, or guitar, now is a great time to do it. These activities are personally enriching. More importantly, efforts to promote personal growth often give people greater hope for the future.
Engage In Art Therapy
Now is also a time to break out your adult coloring books, or, better yet, start with a tabula rasa mentality and create your own work. Art is one of the most therapeutic activities that you can engage in. It’s immersive, cathartic, and relaxing. When you’re focused on drawing or coloring in the lines, choosing complementary colors, and achieving a very specific aesthetic, you cannot simultaneously dwell on all the outside problems that are beyond your realm of control. Creating art in any form can be both meditative and restorative. This is additionally a good time for art appreciation. Take advantage of online museum tours, free or discounted art or cooking classes, and other arts-related resources. Use online videos to start practicing and exploring martial arts, or start reading and writing poetry. Keeping a journal is also a great way to begin organizing your thoughts, analyzing your own emotions, and venting about your personal discomfort among other things. If you ever dreamed of writing your memoirs, the present moment is offering the perfect opportunity.
For those of you interested in using this form of expression and participating in an ongoing exhibition of art inspired by these current times, see the art that is posted on Instagram Hashtag #Cov19_art. I would like to compile the art, poetry, photography and writing into book that documents the psyche of these times and celebrates our perseverance.
Unplug And Unwind
For all the resources, information, and assistance that the Internet is able to provide during this crisis, it can be just as harmful as it is beneficial. This is especially true when people spend too much time on the web, and when they spend too much time immersing themselves in activities and ideas that foster stress. While staying informed is vital, you must limit the amount of news that you’re reading. Nothing is currently so dire that it requires minute-by-minute updates. Set a special time for logging in and gathering essential information from trusted news sources. Then, set a special time for turning your phone off, logging off your computer, and turning off your TV. Whether you have diagnosed mental health issues or believe yourself to be in excellent mental health, too much information can lead to overload and can leave you feeling deflated, detached, depressed, or excessively anxious.
Make Sure That You’re Getting Enough Quality Sleep
Getting poor-quality or insufficient sleep at this time is a bad idea. Not only will this undermine your efforts to maintain good mental health, but it can also lead to a flagging immune system. If you had a nighttime ritual before, try to stick to it. Moreover, don’t try to mute your emotions or lull yourself to sleep with increased indulgence in alcohol. Some areas under quarantine are reporting as much as a 40 percent increase in alcohol consumption since the institution of stay-at-home orders. Rather than promoting good sleep, alcohol actually reduces overall sleep quality, and shortens the amount of time that people are able to remain asleep.
Try reading a book or meditating before going to bed, taking a warm shower, and turning off all electronics and Internet-connected devices. If necessary, sip a warm cup of chamomile tea or a large mug of warm milk and honey. Making deep and restful sleep a top-priority is one the best things that you can do to promote physical and mental health at this time.
Practice Mindfulness And Conscious Directing Of Your Thoughts
No other world event has highlighted the value and importance of mindfulness than the COVID-19 pandemic. With so much going on around you, it can be difficult to not let feelings of anxiety and panic set in. There is enough fear and stress in the present movement to exhaust anyone’s ability to mentally process current world circumstances. As such, there is no need, reason, or benefits in worrying about possible problems that might lie far ahead in the future. Practice focusing on the moment. Enjoy what you have you right now and work on fostering a mindset of gratitude. If you’re tired of being stuck alone at home, remind yourself that there are some people who have no homes to take shelter in. Give yourself permission to only worry about and deal with the problems that you’re immediately facing. Practicing mindfulness can help alleviate negative emotions about past events, while also limiting anxiety about what the future might hold.
The state of your mental health should be a key concern right now. Actively promoting good mental health and proactively protecting your general sense of well-being is critical. With greater mood balance, proper stress management techniques, and a focus on enriching and expanding yourself, you can successfully survive the mental and emotional ravages of this global pandemic, and any other unexpected life events.
Looking after your wellbeing while staying at home
Staying at home for a long time can be difficult, frustrating and lonely for some people. You may start to feel unhappy.
It is important to remember to take care of your mind as well as your body. You should ask for support when you need it.
Stay in touch with family and friends over the phone or on social media.
TIPS FOR PERSONS WITH STROKE / NON COMMUNICABLE DISEASES (NCDs)
Stay at Home
Observe social distancing
Observe personalhygiene
Cover your mouth when sneezing or coughing
Take your drugs as prescribed
Take a lot of water , fruits and vegetables
Speak to a Health professional
if you have any difficulties or call contact center (MoI)311(about restrictions or 112 (about COVID19) Covid19 Info. WhatsApp number 0555311311 or SASNET-Ghana
Think about things you can do during your time at home as a person with Non Communicable Diseases like Stroke, Diabetes, Hypertension, etc
Keep yourself busy with activities such as cooking, meditating, reading, online learning, stroke & NCDs groups like the online Post Discharge Stroke Support (PDSS).
If you feel well enough you can do some exercise in your home or garden, especially aerobics exercises .
Can I get a viral infection after handling a package from someone who was infectious or that was delivered from a country where there is a high caseload?
What are the signs of symptoms of viruses, including COVID-19?
3. How does SARS-CoV-2 cause infection in human pneumocytes
4. What are the contributing factors to more severe disease.
The United States prepares itself for the impact of COVID-19 that will likely be unprecedented. Although we can say that most people who become infected will have a milder disease, we cannot always predict who is at greater risk for a severe outcome. Particular attention goes to healthcare workers, lower-income communities, and people with advanced age and chronic health conditions. To those unfortunate ones who develop severe disease and require hospitalization, the US health system faces shortages of ventilators, personal protective equipment (PPE), bedspace and the even the healthcare workers to attend to them. Worst-case scenarios project hospitals to become flooded with those who have severe disease, particularly if cases were to occur with the same momentum as Italy or China. The hope is that through the social distancing measures recently implemented, we may be able to blunt the outbreak peak and prevent overburdening our healthcare system.
The general audience has had access to many resources on COVID-19, such as the CDC, WHO, health blogs, video posts, and primary literature. As we face this outbreak, never before has the nation’s working knowledge of viral infections been greater. Since the outbreak was declared in December, we have had three months to learn more about this virus.
This post will go one step further into understanding the contributing factors to a viral emergence and how this likely is not the last outbreak we will have in the coming years. What happens when a virus infects our bodies? What occurs inside that leads to a certain presentation of a disease state? Although COVID-19 is shrouded in mystery, it adheres to natural rules, many of which we still need to define. The mechanism by which a pathogen causes an infection is a clue to how it can be defeated.
Viruses are Host and Cell-specific, until they cross species.
Viruses are intracellular pathogens that are species- and cell-specific. This means that they are usually only capable of infecting one animal. Though there may be some fluidity to this concept. A virus can reside in an animal, whether it is actively infecting the animal or not. An animal virusis called a zoonotic virus, and the animal carrying it is a reservoir. In viral zoonotic spread, mammals (e.g. bats, primates, etc) are the most common reservoir followed by birds. When the conditions are right and several barriers are able to be breached, viruses can jump species, infecting other animals including humans. The process by which a virus jumps species and causes human infection is termed a spillover, an example of which is our current COVID-19 pandemic.
Over 75% of new or emerging diseases originate from animals. From 1940 to 2004,Jones et al. (2008) determined that there were a total of 335 emerged diseases, 60% originating from animals. In most outbreaks, human behaviors shaped the conditions that made it possible. The principal factor relates to human encroachment into animal habitats. It is no coincidence that an acceleration of outbreak has occurred in the last sixty years (fourfold increase) in the setting of a massive population boom. Eerily, a Times article describing spillovers written in May 2017 was entitled The World is Not Ready for the Next Pandemic.
“We cut the trees; we kill the animals or cage them and send them to markets. We disrupt ecosystems, and we shake viruses loose from their natural hosts. When that happens, they need a new host. Often, we are it.” David Quammen, author of Spillover: Animal Infections and the Next Pandemic writing in New York Times.
From the 1800’s, it took approximately 127 years for the population to increase by one billion, i.e. from one to two billion, an achievement that only took thirteen year intervals over the last several decades to achieve 7 billion. The population growth may be a driving force for disputes over settlements, habitat invasion, the use of exotic animals as a food source in the setting of growing food insecurity, or the trade and introduction of exotic animals to be used as products or pets. Certain features directly related to the virus, including mutations, deletions and recombination, enable the virus to survive and then flourish within an introduced animal.
Contributing Factors to a Spillover are related to human and animal behavior, as well as ability for the virus to persist in an introduced host.
Although outbreaks are infrequent events, current conditions may allow for an increased risk. For a virus to jump species from an animal reservoir to to human to human spread, usually several conditions would need to be met. First, animals infected with a virus need to be stable and have persistent shedding of virus, while not succumbing to it. Second, the animals would need to be in close proximity to humans. Next, an exchange of infected fluids, such as saliva, mucus, feces or blood, or the ingestion of an animal allows for a sufficient amount of virus to be introduced into the new animal by its usual infection route. While inside the human, some of the virus must possess a specific (enough) receptor mutation to allow for avidity (or connection) of the virus to a host receptor to gain entry into the specific cell. Finally, it must be able to propagate and infect other cells, without being identified and neutralized by the host’s innate immunity. Once it is able to survive and replicate within the human host, it must be able to be transmitted from one human to another. If any of these conditions are not sustained, a spillover does not occur.
Street Light Diagram of Components to A Spillover: Adapted from RNA viruses: a case study of the biology of emerging infectious diseases. Woolhouse M. et al. Oct 2013. Microbiol Spectrum.
From the “Street Light Diagram,” yellow (level 2) is intended to connote caution. Red (level 3) indicates higher risk of pandemic potential, but certain viral and non-viral kinetics (e.g. population density, behaviors) prevent easy transmission. These factors influence the basic reproductive number (Ro), with an Ro of greater than one to allow for risk of exponential growth. The black (level 4) designation is related to epidemic spread. For a detailed list of RNA viruses that are recognized as causing infections in humans and their respective levels, refer to Woolhouse M. et al (list).
Of particular concern are the 180 and counting (2 newly identified per year) RNA viruses capable of infecting humans, the majority (89%) of which are zoonotic. Examples of recent RNA viruses that have emerged include HIV, influenza virus, NIPAH virus and the Coronaviruses SARS, MERS and SARS-CoV-2. RNA viruses may more easily jump species, because of their tendency to mutate and adapt more easily when introduced. Not all RNA pathogens that cause infection in humans from animals are capable of being spread from human to humans. The majority of zoonotic RNA viruses are restricted to level 2 (approx 107 out of 180 species). An example of this would be avian influenza (H5, N2 or H9, N2), which does readily not cause human-to-human transmission. It may be related to the cell type infected, the sialic acid receptor, which is in the upper respiratory tract of poultry and lower in humans. This is fortunate because it has an estimated case fatality rate of 14-30%. Level 3 spread is seen only in about 73 species and spread is limited in 26 of these RNA viruses. The remainder (47 Level 4 RNA viruses) can spread human to human, causing epidemics..
Very rarely,a virus may already be able to adapt to a human and lead to an outbreak, termed “off-the-shelf” viruses. More likely, viruses eventually adapt from repeated animal to human transmission and evolve to be more transmissable between humans (Level 3 to Level 4). HIV probably crossed over from chimpanzees to humans in what is now the Democratic Republic of the Congo in the 1920’s, possibly from hunters who ate “bush meat” or had cuts and wounds contaminated with chimpanzee blood infected with Simian immunodeficiency virus (SIV), a milder disease which does not alter the lifespan of the infected animal. The ability of HIV to cause a prolonged infection and be transmitted via various routes including bloodborne and sexually enabled it to become a level 4 pathogen and reach global transmission.
The SARS-CoV-2 emerged likely from bats with the possiblity of a secondary animal reservoir the pangolin. Bats are known carriers of coronaviruses and have been determined to be the likely reservois for SARS and MERS. Andersen et al. published a recent correspondence entitled the proximal origin of SARS-CoV-2. The authors discusss several possible and contributing scenarios. On account of a 96% identical genome with a sampled bat coronavirus, bats were likely the original reservoir of SARS-CoV-2. However, SARS-CoV-2 may have evolved the protein stucture of the S-spike to allow for better binding to human ACE2 receptors from pangolin through natural selection. It is possible that a polybasic cleavage site (necessary for cell-cell fusion) may have evolved after being introduced into humans.
From Spillover to Infection and Disease
When COVID-19 emerged from an animal source and was capable of human to human transmission, humans had no prior memory of this virus. The immune system was caught off-guard with minimal defense. As a virus infects cells and increases its numbers in the host, the disease develops, a time when a person presents with signs and symptoms. Even in the setting of a novel virus, most of the way a disease manifests is due to the host inflammatory response and not because of a distinct genetics, appearances (e.g. receptor sites) and other characteristics of a virus.
Cell infection
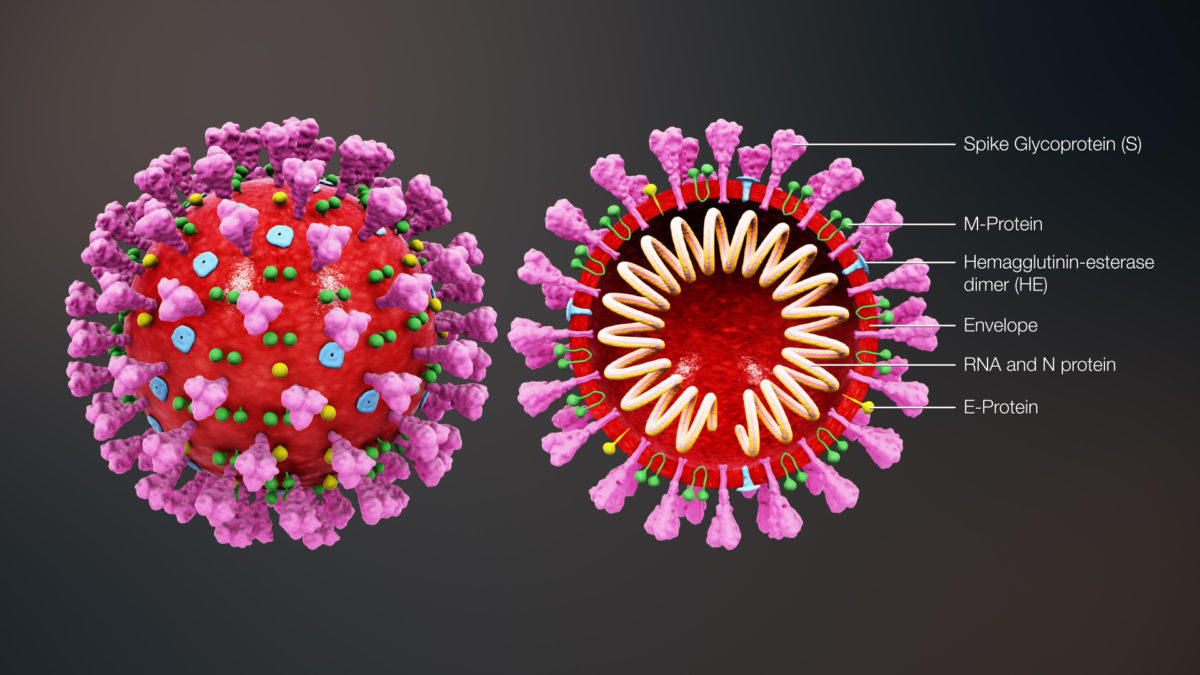
A virus is an obligatory intracellular pathogen, meaning it can only thrive within cells. A specific virus infects a specific type of cell. Hepatitis C virus infects hepatocytes; BK virus infects the transitional cells of the bladder; influenza virus and coronaviruses infect type I and type II pneumocytes in the respiratory tract; HIV infects CD4 lymphocytes and Langhans cells. The specificity of cell-type is not accidental and relates to a lock-and-key mechanism that a virus has with the cell it infects. Think of it as a parasite requiring the mechanics of the host to build more copies of itself. It enters the lining of the respiratory tract and attaches onto cells by means of a receptor interaction. Specifically, this is between an outer membrane receptor of the virus (Spike glycoprotein (S)) and a receptor(s) on the host cell. The virus then enters the cell by a process known as endocytosis.
Upon entry, the virus hijacks the cell’s ability to read nucleic acids and produce proteins. COVID-19 is a positive strand RNA virus, with the viral RNA serving as a messenger RNA, leading to the production of hundreds of copies of virus RNA and proteins in a single cell (known as replication). These copies self-assemble and form multiple viruses, or progeny. This results in stress on the cell and cause changes in the cell membrane (membrane rearrangements), damages the infected cell, and go on to infect other cells.
The extent to which a virus can infect cells in known as its pathogenicity. The speed at which a virus can spread through the body and infect other cells is known as the virus lifecycle. In the case of viruses, typically thousands of copies can be generated in a period of a day and lead to significant inflammatory changes in the body as a response to infection.
ACE2 as a SARS-CoV-2 receptor
The S receptor on the SARS-CoV-2 binds to a specific receptor that lines the cells of the lung tissue, as well as heart kidney, endothelium (the inner lining of blood vessels) and the intestines, known as the Angiotensin-converting enzyme 2 (ACE2) receptor. This interaction is a required step for viral entry into the cell. Using a mouse model, an increased expression of the ACE2 receptor allowed for more viral entry into the cells and resulted in greater disease severity. Further studies will have to sort out the speculation that medications such as ACE inhibitors, Angiotensin receptor blockers (ARBs), ibuprofen, or thiazolidinediones, all of which upregulate ACE2 receptors would potentially worsen COVID-19 disease. As for now, it does not appear to be the case. In the realm of vaccine and therapy options, it remains to be seen if blocking these receptors, for instance through antibody therapies, or providing a vaccine that triggers antibodies to the S receptor would alter pathogenesis of the virus.
How does our immune system recognize these invaders?
The evolution of the immune system occurred in the face of the continuous onslaught of microbes from the environment.The human immune system consists of innate and adaptive immunity.
Innate Immune System
The innate immune system is the first branch to respond to a viral assault. The components of the innate immune system include cells, such as natural killer cells, dendritic cells, monocytes and neutrophils, and complement proteins. The innate system senses changes that occur to the cell from viral products and cell damage (Pattern Recognition Receptors). This triggers the release of interferons (IFN), which promote inflammation (activate molecules known as cytokines) and reduce virus replication. The cytokines signal special cells, known as natural killer and dendritic cells, which destroy infected host cells to reduce the spread of the viral infection. The PRRs also trigger a process known as autophagy, in which an infected cell degrades itself to reduce (or the intent to reduce) further infection.
The complement system consists of several proteins that form a complex, leading to cell breakdown (lysis). They can also signal certain cells such as activated macrophages to engulf infected cells, a process known as opsonization.
Adaptive Immune System
Adaptive immunity requires antibody production and cell-mediated mechanisms. Some natural antibodies may already be circulating for a given virus that can provide some initial immunity (known as IgM class antibodies). These are generated by antibody-producing white blood cells known as B cells. Otherwise specific cells known as Activated macrophages can engulf cells to produce antigen that express more pathogen-specific antibodies by B cells. The dominant antibody types in humans are IgM, IgD, IgG, IgA, and IgE, each of which has specific roles in the immune response. The IgG is involved in the memory responses and form to neutralize a virus.
Another white blood cell line, known as T lymphocytes (T cells), are produced in a small gland known as the thymus, which is inside the front part of the chest (behind the sternum and in between the lungs). These T cells provide cell-mediated immunity. Specific cells are produced that have receptors for a given pathogen and can neutralize them.
From Infection to Disease
When a person becomes infected with a virus or bacteria, there is a period of time at which s/he is symptomatic. The term that is used from onset of the infection and expression of the disease is known as incubation period. Various viral infections have different incubation periods. For instance, influenza’s incubation period is one to four days; COVID-19 may take one to fourteen days (average of 6) to show symptoms. During the prodromal phase, the person develops early symptoms of a viral disease. This could be the beginning of nasal congestion, sore throat, cough and tiredness. After a threshold is reached and enough cells become infected, a more sizable inflammatory response is generated. It is at this time, the person becomes symptomatic.
During the invasive phase, the number of circulating virus intensifies, while the body responds to the infection with a maelstrom of inflammatory markers. The severity of the presentation correlates to the intensity of infection and the inflammatory response. Eventually, the inflammation subsides as neutralization of the virus as a result of the immune system. It is at this point that a person’s symptoms gradually resolve.
Viral Disease: It’s all about inflammation
In approximately 80-85% of those infected with SARS-CoV-2, only a mild disease is seen. In the remaining, a severe infection can lead to hypoxia (low oxygen levels) and need for mechanical ventilation. Owing to increased cellular damage, the subsequent inflammatory response may pose a threat on life.
Risk Factors: In a study of clinical course and risk factors for mortality in COVID-19, risk factors were identified in almost half of the patients, with hypertension, diabetes and coronary heart disease. Smoking likely leads to a two-fold risk of more severe disease than a non-smoker. Advanced age is also a significant mortality risk. From the Wuhan epicenter data: 80+ years, 14.8%; 70-79 years, 8%; 60-69 years, 3.6%; 50-59 years 1.3%. This is likely on account of dysfunctional innate immunity, IL-2 signaling (not down-regulating) and T-cell mediated immune system with aging. What still remains unknown for COVID-19 infection is whether there exist genetic determinants (as seen in other viral diseases) that lead to a greater risk of a more severe infections. This could explain why we are hearing reports of severe disease in the “otherwise healthy” youth.
Pathogenecity and Inflammation Contribute to Disease Manifestations. The extent to which someone presents with more severe disease relates to an interaction of amount of cell destruction from viral burden and host response. Below is a depiction of the contributing effects of Viral Pathogenicity and Host Inflammatory Response in disease. Increased viral infection burden is likely an important contributor to a greater immune response. It may be that type 2 pneumocyte infection in the lower respiratory tract may cause a greater cytokine release than infection in upper respiratory cells.
Disease: A “dance” between viral infection and immune response
Disease Presentation
The most common symptoms on admission were fever and cough, sometimes with sputum production and fatigue. Interestingly, the average time of presentation of respiratory complaints, such as shortness of breath, is approximately 7 days and need for invasive ventilation is 14.5 days (range 12-19 days), suggesting that the latter part of infection may be when greater inflammation develops “cytokine storm”. The most frequently observed complication was sepsis, followed by respiratory failure, ARDS, heart failure and septic shock.
**The shortness of breath (“Dyspnea” in blue) started around day 7 in both groups**
Laboratory Findings for Hospital Management
There is a significant inflammatory response in more severe infections of COVID-19. Patients may develop ARDS, which is the leading cause of mortality. Several findings of the disease support a hypercytokine, hyperinflammatory response that contribute to a more severe presentation. These patients have a persistent fever, low white blood cell count, elevated cytokines (IL-2, IL-7, IL-6, GM-CSF, Interferon gamma and others), an elevated ferritin, and an elevated D-dimer.
Future Therapy
In an unprecedented move, the FDA has granted emergency authorization for the use of hydroxychloroquine along with azithromycin based on early clinical data that there may be a benefit of hydroxychloroquine in reducing viral load and inflammatory state. We await further progress in other therapeutics and vaccine trials, many of which are now underway.
Summary
The COVID-19 outbreak was a spillover event of a novel coronavirus from an animal reservoir that led human to human transmission. Further research is required to understanding the way the infection can lead to various disease manifestations, including who may be susceptible to more severe presentations. Hydroxychloroquine along with azithromycin may provide some benefit in treating those with severe disease. As for now, we await for the results on the treatment and vaccination fronts.
A National Institutes of Health study found the corona virus can live on cardboard for 24 hours and 2 to 3 days on plastic and stainless steel (1). I have not heard anyone sneeze or cough in public since the corona virus surfaced yet it took only days to travel 50 miles to reach my area. The people who load and unload cartons that are delivered are a possible vector for the rapid spread. Shopping while wearing a glove on my sound hand and using a credit card instead of cash (see previous post) was not just paranoia. Thank God I rehearsed because initially I made mistakes.
Initially I grabbed the handle of my car door with the glove I had pushed the shopping cart still on my hand. Whatever was on the glove was now on the handle. Now I can quickly put the glove in the plastic cup in my car door. I made it easier to put the blue foam covering my hemiplegic thumb in an isolated place. The weather got warm so I can no longer put my credit card in my coat pocket. I put the card in a tiny purse and hung it from my big purse. The arrow points to the velcro closure which is easy to open one-handed. The tiny purse hangs in front of my stomach where it is harder for someone to open it without me noticing. homeafterstroke.blogspot.com
During an uncertain time as we realize the impact of the COVID-19 outbreak on the local communities, here are a few questions and answers regarding the virus and ways in which we can reduce spread:
Why is it called novel “coronavirus”?
Coronavirus is named for its appearance of the virus’s outer membrane on electron microscopy, which resemble a crown. These zoonotic (animal derived) viruses were first discovered in the 1960’s and likely makes up approximately 15% of all colds.
The designation of “novel” comes from the fact that the virus is genetically distinct and emerged from animals and was capable of infecting humans, and then made the jump to human to human infection. Scientists call the phenomenon of a virus being able to infect another animal as a “spillover.”
There are four major strains of coronavirus that cause common colds during the respiratory virus season. COVID-19 is different from these in that it possesses different features on the viral outer layer that is foreign to our immune system.
Our bodies come across viruses frequently and our bodies have innate (meaning built-in) and adaptive (developed) mechanisms to protect us from them. With COVID-19, the virus has not circulated in humans before, so the protections that normally dampen the response to infections are not present.
Therefore, there is an imbalance of managing this, resulting in increased viral stealth and an increased inflammatory response. The body knows something is wrong but it cannot temper the response. A mixture of these interactions contribute to varying severities of infection that could lead to a threat on life.
How is a virus spread?
Like most respiratory viruses, COVID-19 is spread in respiratory droplets. Just to illustrate the magnitude of spread, take one simple cough. One cough can spread thousands of droplets into the air at up to 50 miles an hour for 6 feet. The size of the droplets measures from 10 microns to 100 microns. Just to give you an example of size of 10 microns, it would 100 droplets of this size together to make it visible (e.g. 1mm). If the virus is 100 nanometers (or 0.1 micron) a droplet can have from 100 to 1000 viruses riding within it. A single cough then is capable of shedding millions of copies of a virus.
How far the droplets can be spread depend on their size and wind currents – the majority of which fall within six feet, the space that doctors advise for social distancing. There is no compelling evidence that the virus is easily transmitted in the air, or airborne. Likely, as with all viruses, there is a continuum. Small droplets known as droplet nuclei can travel on air currents for longer distances or float in the air. Although people likely have a personal cloud of droplets around them, it is unlikely that this virus can be transmitted easily beyond 6 feet.
Studies have demonstrated that COVID-19 can remain viable, or “infectious” for 2-3 days and perhaps several days on surfaces. This is not likely to constitute the main mechanism of spread and is also not unlike other respiratory virus characteristics.
The important thing to communicate is that the virus operates by natural laws and although new to our immune system, as we gain greater information of its mechanisms and employ rapid testing to mitigate risk and target containment, the chain reaction that is this outbreak can be blunted and interrupted.
How can I prevent the spread or protect myself from a virus?
General measures are still helpful to try to reduce the risk of getting this virus. Respiratory viruses notoriously difficult to protect against. The CDC estimates that between 10 million and 50 million people get the flu yearly. Nevertheless, an increased vigilance in these practices may still provide some protection:
Good hand-washing with soap and water for 15-20 seconds or the use of alcohol-based sanitizers
Social distancing and avoiding anyone who is coughing or sneezing. If you are sick, ensure that you are practicing measures of social distancing, handwashing and sneezing/coughing into your arm sleeve and not shaking hands.
“Corona elbow-bump” or ankle hit, instead of shaking hands. These are now “in” and accepted ways of showing respect, acknowledgement and affection.
Avoid touching the face, nose, eyes or mouth, which could lead to ingestion of the virus particles.
Wipe contact surfaces down before and after use, e.g. in the gym or in a common area or avoid touching your face or washing your hands after use.
Wash you hands before preparing food and before eating.
Can I get a viral infection after handling a package from someone who was infectious or that was delivered from a country where there is a high caseload?
COVID-19 is predominantly spread by respiratory droplets, where millions of viruses can be spread in one cough. As other respiratory viruses, it can be transmitted by shaking someone’s hand who is infected and had coughed, sneezed or touched his/her face, touching a contaminated surface or an inanimate object (fomite) that have infected respiratory droplets.
It is unlikely that the virus can survive on absorptive surfaces such as cardboard for very long or in packages for longer than several hours, so it would be unlikely that the virus could be spread effectively in this fashion. Some studies of coronaviruses (including those that cause the common cold) as well as other the coronaviruses SARS and MERS have shown that viruses are capable of remaining infectious for 2-3 days, and in some cases several days. Fortunately, they are easy to wipe off with alcohol-based solutions, dilute bleach and other cleaning solutions.
If a delivery person is dropping off a package and is infected, there is a conceivable risk of transmitting viruses, if he/she coughs or sneezes on the package. This is an exceedingly low risk to the general public. Handwashing throughout the day is always recommended during the cold virus/flu season, in addition to avoiding touching the face, eyes or nose when out in public.
What are the signs of symptoms of viruses, including COVID-19?
Respiratory viruses infect mucosal surfaces in the respiratory tract, usually from nose to bronchial airways and sometimes even the lower respiratory tract. The more severe presentations are seen where a virus causes damage to the respiratory tissue, a process known as viral pneumonitis or viral pneumonia. Many viruses can cause this type of infection, including influenza, adenovirus, respiratory syncytial virus and COVID-19.
The common cold mostly causes cough, nasal congestion or runny nose and possibly a sore throat. It is not uncommon to have some tiredness and low to high temperatures for any of the respiratory viruses. Some people will have nausea and diarrhea.
The most common symptoms of COVID-19 include fever, cough and tiredness. If you have these symptoms, you would not be able to know if this was COVID-19 or another respiratory virus, without a specific test, a PCR on nasal secretions.
Most people will have only mild to moderate symptoms from COVID-19 that will improve after a few days of staying home, resting, keeping well hydrated and nourished. In those that are of advanced age and/or who have high blood pressure, heart disease, lung disease or diabetes, they may have a worse presentation that may require advanced care, including hospitalization. A smaller amount will die from the disease.
If I have a viral infection, when should I go to the emergency department or clinic?
The concern of severity of infection can get anyone worried about their health. We hear daily the amount of those that have died from COVID-19 and not influenza. The CDC estimates that as many as 30,000 people have died in the United States from influenza this season 2019-2020.
If you are experiencing cold symptoms that are minor, that is you feel tired and achy and are coughing a little, you can stay home and allow time to recover. If you are experienced a fast heart rate, recurrent fevers and increasing problems with breathing – “catching your breath”, “having difficulty breathing” or being “concerned about my breathing” are key words – then you should seek further care in your local emergency department.
We are currently not screening everyone with cold symptoms, reserving this for those who have severe enough illness to be hospitalized for now. With the amount of cases now reported in the community, there is likely local spread. Nevertheless, in people that are being tested, various viruses are likely to show up, like influenza A/B, respiratory syncytial virus (RSV) and metapneumovirus. With the upscaling of testing, it is likely that we may be able to test even those that have mild to moderate symptoms to better address the outbreak and target quarantine measures.
Unless your symptoms are as described above, it is recommended not to go to the local clinic or emergency department, where a respiratory virus could get transmitted to those that have chronic heath conditions and at risk to have more severe infection.
What should I do about my travel plans?
With the report of cases of more than 1400 cases in the United States (March 12, 2020), families are beginning to wonder if they should change their spring break or other trip plans. The United States has enacted nationwide measures and various states have declared local emergencies to protect the public. Large events are being canceled as a means of interrupting viral transfer in the name of social distancing.
With this increased awareness, families are trying to balance between canceling plans to protect themselves or following through with the plans and possibly putting themselves at risk or contributing to further spread. The spread of disease in this outbreak is extremely volatile and could require in a sudden shift in plans as events are canceled.
The following are some considerations for your decision:
Did you purchase travel and/or flight insurance?
Is your ticket purchase (e.g. an amusement park) only for “same day” or can it be transferable for a later time? Review all of the policies for cancellation of the event, and contact the venue, park or hotel to discuss exceptions,etc.
How flexible are you to the possibility of sudden changes in your plans?
As for the risk of attending these events: The risk of acquiring any respiratory virus is increased with proximity and likelihood of coming into someone who is infected, such as in social activities. Common practices of social distancing and avoid contact of infected surfaces or inanimate objects (fomites) cannot be assured in an amusement park, for instance. The same is true with access to hand washing.
Here are a few measures that families can take to prepare themselves for their trips:
Have hand sanitizer and handwipes available for use while traveling.
Instruct children to cough and sneeze into their sleeves and not their hands – and other practices to avoid touching the face, nose or eyes.
Check on outbreak information at the specific location or closest city to it before you embark. Disney just announced today that it’s closing the California park because of COVID-19.
Families can take certain precautions in advance of surprises. COVID-19, as with other respiratory viruses can have a major effect on people of advanced age or with chronic conditions such as hypertension, heart disease, diabetes and lung disease or who are immunocompromised. The majority of travelers require no further preparation than what they would do to protect themselves from viral infections during the cold season.
I hope this information is found to be useful. Please share this with your friends and please feel free to comment. This will be placed in the Health Information section as well as COVID-19 resources. Thank you for reading this.
The novelty of the novel COVID-19 outbreak has passed. Sure our imagination that drums up images of viral apocalypse and global chaotic destabilization are simmering. Although the fears are transforming into measured preparedness, there still remains an allure of uncertainty with how this outbreak will affect the rest of the world. In the wake of this recent outbreak, the global public health community and the world in general is left with many important questions. In real-time, the community has had to develop a blueprint to testing, containment and risk mitigation. While the United States and countries in Europe are reporting higher case loads, some important lessons can be gleaned from the early part of the epidemic:
Emerging Lessons:
Containing the Transmission of a Respiratory Virus is like trying to hold water in your hands.
When the nCoV-19 (COVID-19) outbreak was declared in Wuhan, China in late December 2019, about three weeks of potential transmission for the index cases had occurred. The first wave of cases were close contacts and healthcare workers. The virus was transmitted to others through coughing, sneezing, talking, kissing, or from contaminated surfaces or objects.
Just one cough sends out thousands of respiratory droplets, varying from 10 to 100 microns in size, at a speed of 50 miles an hour to a distance of a meter or more. If you sneeze when you have the cold, you are sending out 40,000 droplets of 0.5 to 12 microns at a speed of 100 m/s. Imagine that if viruses, such as COVID-19, are 100 nanometers (0.1 micron), hundreds can surf on these droplets and easily become sprayed onto objects or surfaces at a closer distance, while droplet nuclei (<5 microns) may spread distances of a few meters or may even follow air currents still further.
These infectious secretions can easily then enter the mouth, nose of eyes of a passersby or get ingested after touching the face from surface or fomite transfer. Studies support the concept of a “personal cloud” of infectious particles supplied by coughing and sneezing and air currents around an infected person. With so many viral particles, transmission of an infection to multiple people becomes easy.
The Wells evaporation-falling curve of droplets From Annex C. Respiratory droplets.
2. Case Fatality Rates (CFR) are always overestimated in the beginning of outbreaks
An outbreak requires constant reassessment. Imagine trying to isolate and contain an outbreak, while at the same time trying to identify the pathogen, confirm cases, protect those at risk, and consider treatment and vaccination options – all in real time.
Epidemiologists can draft a case definition early on, but if the outbreak is from a novel pathogen, cases are defined by syndromic presentation first until more specific tests become available. The public health system and the general public have sensitive ears for case fatality rate, the amount of those dying from a specific infection over the amount of those infected.
Case fatality rates (CFR) depend on knowledge of all affected cases, which for respiratory virus is usually not possible. The problem is that most patients that have mild infection may not get tested. On the other hand, some serious cases may not go attributed to the infection. As we are learning, even later into the outbreak, e.g. in the US, outbreak investigation and containment largely depends on the availability of tests kits.
In China, the Wuhan COVID-19 outbreak had an attributable CFR of 4%. These original rates are higher than what has mostly been seen in secondary outbreak countries, such as South Korea. One-third of the caseload was determined by syndromic definition rather than specific testing. Many more may have not been tested. The more people that are tested including those mildly symptomatic or asymptomatic, the closer we get to understanding the true CFR.
Enter South Korea. When COVID-19 was reported in South Korea, great strides were made to identify cases. On Tuesday March 3rd, Moon Jae-in declared “war” on COVID-19. This comes after an outbreak of MERS in South Korea where tests kits were not readily available, and 38 people died. By March 4th, South Korea has already tested more than 140,000 people for COVID-19, even providing a “drive-through” testing option. South Korea has detected 6,593 cases with 43 total deaths.
If you take into account a sensitivity of 95%, there may be 5% false negatives, this would equate to a CFR of 43 deaths/6,593 x 100% = 0.65%. This represents the unadjusted CFR based on the positive tests. However, there is a false negative rate of 5%, so taking into account all of those tested (158,456 – 6,593), the adjustment could be as low as 0.2%. Although there is a possibility that the numerator may not be correct, it is less likely to shift, as there isn’t another definition for “death” but it could not capture the attributable deaths from COVID-19.
The WHO declared that the case fatality rate of COVID worldwide has been 3.4%, which appears to be an gross overestimate. However and importantly, even with the calculated CFR from South Korea, the rate is likely to be twofold higher (or greater) than what is encountered with seasonal influenza yearly. When determining risk, the Wuhan data closely correlated advanced age and those with chronic diseases with increased CFR. So the adjusted case fatality rate is likely to be higher in these at-risk groups and lower in the general population.
*This is coming from the China outbreak – Expect a similar mortality distribution though needs adjusted from other underlying risk factors
Think of a virus as a chain reaction. Anytime a virus can spread easily and only cause some deaths, sometimes considered a “sweet spot” in disease transmission, it is likely to have a significant impact. When a virus kills off its hosts too quickly or is transmitted by a different route (e.g. Ebola with infected blood and secretions), it is impactful in its severity, but it can’t get around to infecting too many people. The CDC estimates that influenza causes about 10,000 to 60,000 deaths annually (CFR 0.1%) – in the Unites States alone. Even if the CFR for COVID-19 similar to influenza, widespread disease could be impactful on our elderly and other at-risk groups and strains health care delivery.
3. Outbreak Containment and Risk Mitigation Strategies Benefit Greatly from Accurate Case Definition
Efforts to contain COVID-19 improve as the case definition becomes more specific. The original CDC case definition was more rigid, since the outbreak was related to the specific outbreak city, Wuhan. As is always the case, coming up with an accurate definition up front can be difficult in real-time. The Chinese government imposed strict lockdown measures, which crippled the cities and was meant to interrupt further transmission. It became apparent, that low grade transmission and milder cases continued both inside China and to other countries.
Chinese scientist defined the genome of the novel Coronavirus shortly after declaring the outbreak, allowing for the development of testing. Once testing became available, it was as if an invisible menace could be seen. In the South Korea outbreak, people were readily tested, so active recommendations for quarantine could be given. Truly it is important to recognize the efforts of the South Korean government and medical community to contain and test the population. This testing may have contributed to the lower case fatality rates, by identifying at-risk people and keeping them free of disease.
With the further spread of COVID-19, a country will be able to gain a greater control on the outbreak through greater testing. This provides knowledge of active cases, so that voluntary quarantine can be put into affect.
4. ProtectingHealthcare workers, Care givers and High Risk Populations is a key strategy
With the SARS outbreak in 2002, we were reminded that the ability to provide healthcare relies on its personnel. During that epidemic, one-fifth of all cases were healthcare workers. As the outbreak of COVID-19 continues, some people will require medical attention and report to the hospital – maybe not even knowing that they have the disease.
As the caseload increases in the United States, the at-risk definition will increase. It may be necessary to wear personal protective equipment with anyone who exhibits a viral infection. Healthcare workers will be a greater risk of acquiring the illness. When healthcare workers are unable to attend to patients because they are sick, healthcare delivery is consequently impacted.
It is clear that there is a higher case fatality rate with the elderly and those with health condition. When an infected person, whether it is a healthcare worker, patient or visitor comes into a population of those at risk, you see a perfect storm for severe disease and fatality. Recently, the Life Care center in Kirkland, Washington had a spate of 13 deaths from COVID-19. it is incumbent on long-term care facilities to develop strategies to prevent any further outbreaks of COVID-19 in such high-risk settings.
5. With any viral spillover, there are always two outbreaks: Infectious Disease and the Infectious Fear.
An outbreak is an unpredictable process. It can sometimes burn out, even as we are still learning of the risk factors of its spread. As for a respiratory virus outbreak, it is easily transmitted, often leading to relatively silent spread. Containment strategies are often too late. As information emerges from the virus, speculation can create narratives that lead to fear, panic and rapid decision-making.
Reports from the news are often related to deaths and how the viral infection is changing regular life and can be sensationalistic. Online authors and presenters are shaping the news and narratives. The images of the strict containment measures in China tempt us to think about self-preservation from an unknown invader. These fears shape behaviors: cancelling flights, stocking up on masks, cancelling conferences. While it is not wrong that containment measures can help, defining cases can lead to more targeted containment without crippling the flow of a functioning society.
In the unknown of the COVID-19 outbreak, the stock market has seen great losses and is showing volatility. Imposing mass quarantine and containment efforts can have real effects on the economy and productivity. Canceling major conferences can lead to losses that can affect multiple sectors. Even if you decide not to cancel your European trip, strict measures could be applied in the setting of an outbreak, that can limit or spoil your vacation plans.
Stories of vampires, werewolves and zombies go back hundreds, if not thousands of years. The concept of some unknown force overpowering humans and causing them to morph into someone or something else hits the nerve of our self-preservation instinct. In many ways, viruses are the true vampires. They are lifeless forces other than the primitive instincts of self-preservation and self-generation. A virus’s consciousness is generativity – producing copies to transmit to others. It’s result is a destructive untangling of the fiber of society. A virus is transmitted through social interactions and an interruptions in these behaviors although may be useful, often results in a significant fallout.
A Viral Outbreak Creates a Fissure in Human Collaboration Efforts, leaving a wake of economic and sociopolitical fallout.
Future direction:
The use of already existing apps for description of symptoms to determine places for targeted testing.
The coordination of an international outbreak system either through already-arranged WHO or influenza surveillance sites.
Selecting specialized labs to launch testing as early as possible.
More rapid protocols for vaccine development in emergency situations that do not require the rigid testing phases as those that are currently imposed by the FDA and other entities.
Summary
Managing the COVID-19 outbreak will require a group effort to stay aware of our individual symptoms and use standard precautions, to identify cases through rapid testing, to mitigate risk through targeted containment and to transform fears into preparation.
A viral outbreak in many ways is like a natural force. The transmission
At present, with multiple people testing positive, COVID-19 has hit several areas in the United States. Do we need to be concerned about this.



























 The Wells evaporation-falling curve of droplets From Annex C. Respiratory droplets.
The Wells evaporation-falling curve of droplets From Annex C. Respiratory droplets. *This is coming from the China outbreak – Expect a similar mortality distribution though needs adjusted from other underlying risk factors
*This is coming from the China outbreak – Expect a similar mortality distribution though needs adjusted from other underlying risk factors